Latest Posts

The Complete Property Transformation Guide From Lot Clearing to Greenhouses and Outdoor Lighting
Transforming a piece of land into a functional, attractive, and productive property takes more than a few quick upgrades. It requires planning, coordination, and the…

A Family’s Guide to Understanding Alcohol Rehab Facilities
When a loved one is struggling with alcohol addiction, families often feel overwhelmed, confused, and unsure of what steps to take next. Learning about treatment…
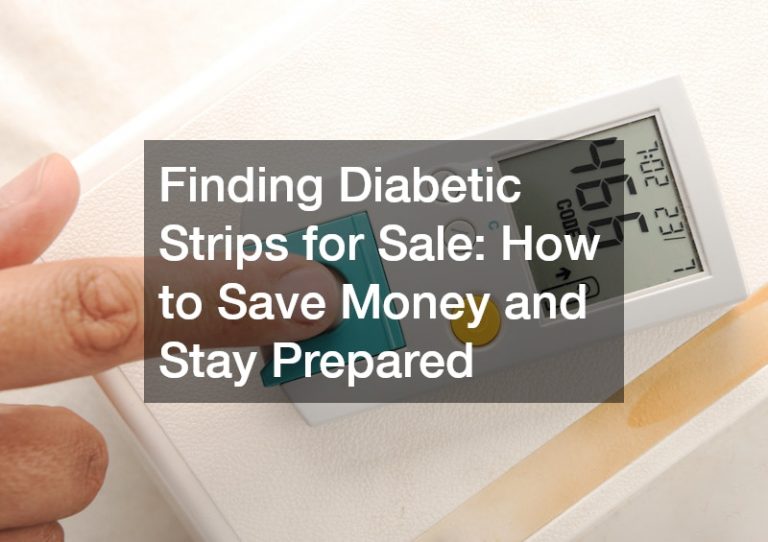
Finding Diabetic Strips for Sale How to Save Money and Stay Prepared
Managing diabetes effectively is hugely dependent on regular monitoring of blood sugar levels, making an adequate supply of diabetic test strips crucial. The importance of…
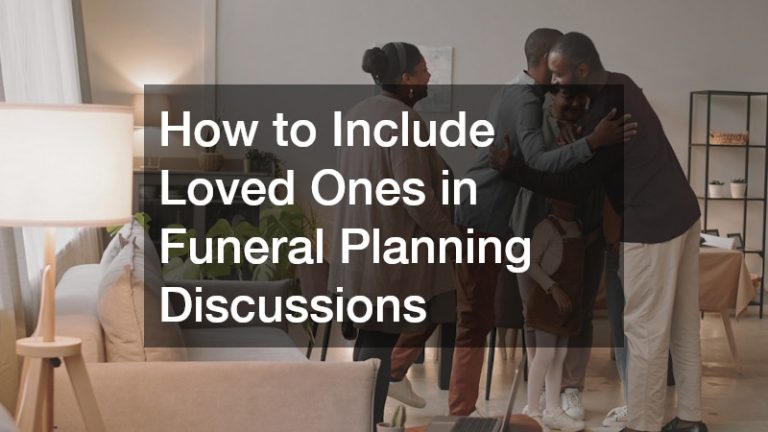
How to Include Loved Ones in Funeral Planning Discussions
Planning a funeral is one of the most sensitive and emotionally challenging tasks a family can face. These discussions often bring up grief, uncertainty, and…
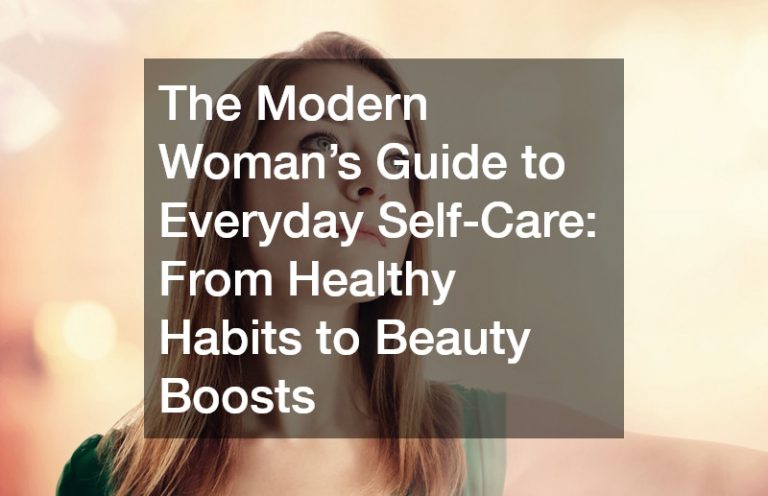
The Modern Woman’s Guide to Everyday Self-Care: From Healthy Habits to Beauty Boosts
In today’s fast-paced world, women are juggling demanding careers, family responsibilities, social obligations, and personal goals. With so many pressures, it’s easy for self-care to…
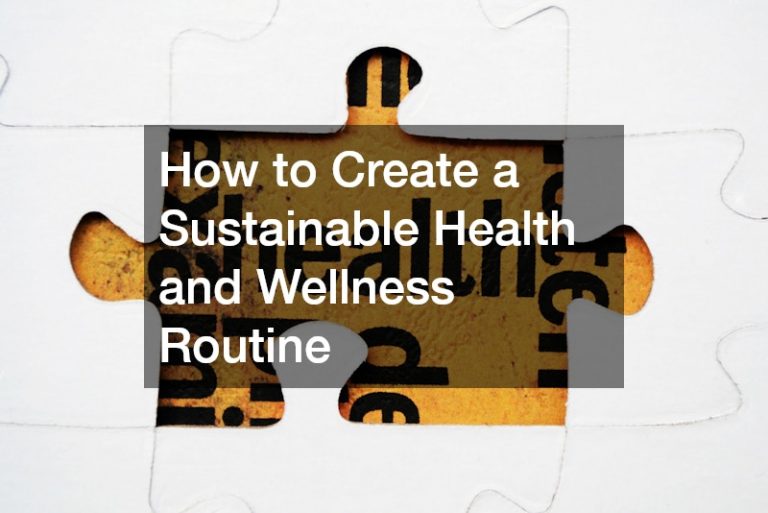
How to Create a Sustainable Health and Wellness Routine
Creating a sustainable health and wellness routine is one of the most impactful decisions you can make to improve your quality of life. Unlike quick…
Editor’s Picks

5 Tips to Ensure Optimal Health As a Woman
Regular health check-ups are key for preventive care. Maintain a balanced diet with ample fruits, vegetables, lean proteins and whole grains. Get at least 30…

How to Make Men with Long Hair Look Professional
It’s a rule in most workplaces not to allow men with long hair in the office. Men with long hair are often seen as unprofessional…

Understanding the Meaning Behind Gifting Jewelry Items
People often give gifts, especially to their loved ones, friends, and other people who are close to their hearts. The act of gift giving is…